After the hullabaloo on Friday regarding AbbVie’s suspension of the ABT-199 trials following not one, but two, unexpected deaths from tumor lysis syndrome (TLS), a few people asked what is this condition and what causes it?
In simple terms, lysis is a medical word used to describe the break up or breakdown of cells – whether through decomposition, destruction, or dissolving. Thus, we have hemolysis, which is the destruction of red blood cells with the release of hemoglobin.
Tumor lysis, however, is a medical emergency whereby the sudden production of massive amounts of potassium, phosphate, and nucleic acids into the systemic circulation overwhelms the body’s garbage disposal units, the liver and kidneys. Urgent hospital treatment is usually required, often diuretics can be helpful to flush out and dilute the excess potassium (too much can slow or stop the heart beating), but sometimes kidney dialysis is also needed to speedily remove the excess production of the potassium. Death can unfortunately (but not always) result.
TLS is most common in aggressive, fast growing (high grade) lymphomas and acute leukemias (e.g. ALL), but is less common in indolent disease such as chronic lymphocytic leukemia (CLL).
Given that AbbVie were testing their Bcl2 inhibitor in CLL, where TLS is rarer, some might think two deaths from TLS a surprise, especially given the positive results reported at the recent American Society of Hematology (ASH) meeting in December (more about the ABT-199 data).
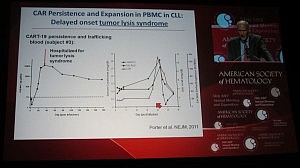
This is not the first time TLS has been reported in leukemias though. Carl June (U Penn) presented the data on their chimeric antigen receptor therapy (CART), a collaboration with Novartis, in CLL and also childhood acute lymphoblastic leukemia (ALL) at ASH. Their lead therapy, CTL019 (formerly CART19), also leads to TLS in both ALL, where it is more common, and CLL patients, although he did state in the Ernest Beutler lecture that the patients received urgent renal dialysis and recovered.
Interestingly, Dr June described the TLS as occurring not immediately, but delayed until 20-50 days post infusion. Given what we know about autologous cellular immunotherapy, a delayed response is not a surprise, but in line with our scientific knowledge to date, since it takes a while post apheresis to activate the T-cells.
You can see from Dr June’s slide that the serum levels of creatinine and uric acid spiked around day 20, but the patient was hospitalized for TLS a few days later:
It is possible that the TLS occurs in CLL as a result of rapid efficacy and on target effects – in other words, the treatment is doing it’s job of killing the cancer cells, perhaps a little too well.
Final thoughts…
We will have to wait and see what happens with the larger randomized phase 3 trials for both ABT-199 and CTL019:
We don’t yet know whether the effect in ABT-199 is a dose-schedule issue or a compound structure issue (especially given the reformulation from the original navitoclax molecule).
If TLS is a persistent toxicity issue and efficacy is durable, then it may well limit both potential treatments to Academic centers with experience and resources to quickly monitor and treat such sudden events in future.
These are exciting molecules but care is clearly needed in managing the toxicities.
Contrast these approaches with ibrutinib, a tyrosine kinase inhibitor that targets Bruton Kinase, where the effects appear to be slow but steady inhibition of a key target driving CLL proliferation. TKI therapies are very Community oncology friendly in comparison, particularly for indolent diseases. Although the Bcl2 and CART therapies look very promising, they may need a more careful and judicious approach to reduce the risk of sudden deaths from TLS.
Since the pre-ASH review of what might be hot at the conference, a few people have written to me asking for a rundown on my highlights from the recent hematology and breast cancer conferences. In the end, I only made it ASH in person, but followed the tweets and news that flowed out of the AACR SABCS meeting, which will post either later today or tomorrow.
Here are a few observations that struck me from ASH. There were some genuine highlights from this meeting, both in lymphomas and leukemias:
Rituximab (Roche) was the only clinical abstract selected for the plenary session this year. I loved Dr Anas Younes’ summary of this data on his Facebook Page:
“Clearly, early treatment with rituximab improved the progression free survival and time to next therapy. It is too early to see any effect on survival. My guess is that watch and wait will disappear as patients and doctors will start recommending early use of rituximab instead of watch and worry!”
The results are therefore potentially practice changing and it’s good to see positive data in a difficult to treat subset.
Ponatinib (Ariad), a third generation tyrosine kinase inhibitor (TKI) had excellent phase I data in relapsed/refractory chronic myeloid leukemia (CML), both with and without the T315I mutation. The phase II trial (PACE) is now enrolling and it is my hope that patients who find the existing TKIs fail or develop the T315I mutation will have a new therapeutic option in the not too distant future if the results continue to hold up.
Brentuximab vedotoxin (Seattle Genetics and Millennium) was the real star at ASH this year though. We’ve covered some background on the blog here. Basically, it’s a novel conjugate consisting of a monoclonal antibody with a chemotherapy molecule bolted on. The data in Hodgkin Lymphoma (HL) was absolutely stunning and a nice follow up to the article published in the NEJM by Dr Anas Younes et al., earlier this year. The companies have since announced that they intend to file with the FDA in early 2011, so perhaps we might see this exciting agent approved in the second half of next year.
Unfortunately, there were also some disappointing lowlights:
Lenalidomide (Celgene) had some interesting data in several phases of multiple myeloma, but what shocked many observers was the results of the MM-015 trial. This was the third study to suggest that there may be a risk for secondary cancers with Revlimid. Previously, the data emanated from the IFM and CALGB cooperative studies, but this was the first company sponsored trial that may be considered a registration study.
Clearly, the trend is not good news at all, although it is known that:
Alkylating treatment for AML and NHL run the risk of secondary cancers later in life
The literature suggests that all three cancers have a higher risk of secondary cancers developing, which may or may not be drug related.
In the light of all this, the myeloma finding with Revlimid is not entirely surprising but one can see why investors panicked and sold off stock after the data was announced. Of note though is that patients in the maintenance arm (MPR-R), however, will clearly receive more exposure to the drug than those in the MPR arm, potentially exposing them to a slightly higher risk.
Bosutinib (Pfizer) is a 2nd generation TKI in phase III development for newly diagnosed CML. Much of the expectation surrounding this agent was whether is would be superior to imatinib (Gleevec) in terms of efficacy in the same way that nilotinib (Novartis) and dasatinib (BMS). Both have proven to deliver earlier and deeper responses than imatinib, albeit with the caveat that we won’t know whether survival and overall outcomes will be better until the 5-10 year data is available. There was also some suggestion from Pfizer evolving over the last year that bosutinib might also be cleaner given that it only inhibits BCR-ABL and Src and not other off-target kinases such as PDGF. Unfortunately, that turned out to be a complete misnomer.
Dr Carlos Gambacorti-Passerini (Milan) did an excellent job trying to put a positive spin on the data, but this was a resoundingly negative trial. The primary endpoint of confirmed complete cytogenetic response (CCyR) at 12 months in the intent to treat (ITT) population was not met, although the secondary endpoint of major molecular response (MMR) was met. The side effect profile was particularly disappointing with a lot of diarrhoea, nausea and vomiting being frequent and most unwelcome side effects, which are very similar to chemotherapy. Much of the goal of targeted therapy is to hit the cancer cells for six while leaving normal cells largely alone. Chemotherapy is highly untargeted and hits everything in it’s wake, leaving people well aware that they are undergoing treatment for cancer rather than living with a chronic condition. Sometimes a disconnect between scientific theory and reality happens.
Pfizer announced at the meeting that they plan on pursuing an EU filing, but would hold discussions with the FDA about the relapsed/refractory setting, suggesting they will not file in the US for newly diagnosed CML, unless the FDA do a U-turn on the secondary (MMR) endpoint. The chances of that are rather slim, I suspect. I’m not entirely sure how the filing might be suitable for the EMA and not the FDA, unless the primary endpoints agreed with the Health Authorities were different. That said, given the good choices already available to people with CML, bosutinib is not going to appeal to many, I’m afraid. Certainly the CML KOLs I spoke to at the meeting were largely unenthusiastic about the agent.
Like many of the attendees, the thing most remembered from Orlando will be the bitter cold, both outside and in the presentation halls! Overall, it was really a rather quiet meeting this year, except for the excellent data in brentuximab.
The annual American Society of Hematology (ASH) meeting has come around all too quickly this year and starts today in Orlando.
I’ll be tweeting snippets from the event (wifi permitting) and also curating the tweets from the event below for those following remotely, based on the official Twitter hashtag #ASH2010, as well as other likely ones that may be in use.
The ASH organisers have a Twitter account (@ASH_Hematology), if anyone is interested in following them. They seem pretty helpful and responsive.
If you have any questions about the scientific presentations at the meeting, do feel free to tweet me or add them in the comments below. I’ll do my best to answer them or find someone who can.
Dr Anas Younes (@dranasyounes), a lymphoma specialist from MD Anderson, will also be tweeting and he has posted some of his top abstracts on his awesome Facebook page – check it out here.
To follow the meeting tweets, click on the play button below. The event runs through from Friday 3rd until Tuesday 7th.
Here’s my 2010 list of a few pipeline and approved products that I’ll be watching out for at the upcoming American Society of Hematology (ASH) meeting , which begins tomorrow and runs over the weekend. Some of them will not the expected hot ‘news’ items so beloved of the medical media who often seem to delight in over-hyping things.
Saturday and Sunday typically embrace the posters, education and plenary sessions, while Monday and Tuesday heralds the oral sessions.
In no particular order, and by no means extensive, these are agents I personally find interesting and worth checking out at the meeting:
1. ARRY-520 (Array Biopharma)
There is still no cure for multiple myeloma, although a wealth of new therapies and combinations has definitely improved survival and outcomes for this disease. It is always good to look out for new agents in development in the relapsed/refractory setting.
ARRY-520 is interesting because it’s a kinesin spindle protein (KSP) inhibitor. KSP is required for cell cycle progression through mitosis and inhibition of KSP has been shown to induce mitotic arrest and cell death, in a similar fashion to taxanes and vinca alkaloids. The company has a number of small molecule compounds in development for cancer:
ARRY-520 has been researched specifically in hematologic models such as myeloma, so this will a poster I’ll be looking out for.
What I love about this compound:
While ARRY-520 may target the spindle like taxanes, it appears to do so without the associated peripheral neuropathy and hair loss.
I wrote about the recent promising data from the NEJM by Dr Anas Younes and colleagues. At ASH the same group are presenting on SGN-35 in relapsed/refractory Hodgkin Lymphoma including adverse events and ORR (Mon 6th, 7am) and another group is looking at the agent in Anaplastic Large Cell Lymphomas (Tues 7th, 7.30am) where they will be presenting data on complete remissions.
What I love about this compound:
The concept of a monoclonal antibody combined with chemotherapy as a drug conjugate is an exciting new disruptive biotechnology with a lot of promise.
3. CAL-101 (Calistoga)
Most (but not all) of the other PI3-kinase inhibitors in development seem to have been focusing primarily on solid tumours with mixed results to date. There is also a potential role for the delta form of PI3 kinase inhibitors in B-cell signalling, which encompasses Non Hodgkins Lymphoma (NHL), Mantle Cell Lymphoma (MCL) and Chronic Lymphocytic Leukemia (CLL). Calistoga have been looking at CAL-101 specifically in hematologic malignancies and 7 abstracts are being presented this year either alone or in combination.
What I love about this compound:
When everybody zigs, zag.
4. Crizotinib (Pfizer)
This year, we’ve all heard a lot about ALK rearrangements in non-small cell lung cancer (NSCLC), but such translocations also occur in anaplastic large cell lymphoma (ALCL). It would be most logical to see if crizotinib has any effect in these people with this uncommon form of lymphoma, so I’m looking forward to seeing what the data looks like in the poster session on Sunday evening. I’m expecting/hoping it will show some positive signs in this particular subset who are chemorefractory.
What I love about this agent:
It’s highly and specifically targeted to ALK, a constitutively active translocation (and occasional mutation) that appears to be driving some lung cancer, lymphoma and other rarer cancer subsets.
5. Imatinib/nilotinib (Novartis)
How low should you go? It is now clear from the evidence that people living with CML who attain a major molecular response (MMR) are less likely to relapse than those with a complete cytogenetic response (CCyR).
Ten years ago, the expected life span was only 3-4 years. Imatinib has dramatically shifted the paradigm for the treatment of CML, with people having a realistic goal of living for at least a decade after diagnosis with early chronic phase disease. It is likely that the baton will soon pass to the new second generation TKIs such as nilotinib and dasatinib, which can help achieve an earlier response into the ‘safe haven’ zone. They typically all achieve 90% response rates, but differ in their side effect profiles owing to the additional targets they inhibit.
It will be interesting to see what new data will be presented at this meeting in the annual IRIS trial update and other presentations in several sessions on Monday 6th.
What I love about this drug:
You can’t keep an old warhorse down!
6. Ponatinib (Ariad):
None of the TKIs currently approved for CML target the rare T315I mutation, which ponatinib does target, based on preclinical data. Initial phase I data in the relapsed/refractory setting including T315I mutations is due to be presented in Orlando in the oral session (Monday 6th, 8:15am).
What I love about this compound:
Resistance to all of the TKIs is not that common in CML, but I do think it would be good to have an option for those who find themselves in that unfortunate situation.
7. Rituximab (Roche/Genentech):
Most of the plenary presentations on Sunday afternoon are scientifically focused this year, but there is some preliminary clinical data on rituximab in follicular lymphoma (FL).
The randomised trial from the UK looks at rituximab versus a watch and wait strategy in patients with stage II, III, IV, asymptomatic, non-bulky FL. The reason for this is that patients with asymptomatic, advanced stage, follicular lymphoma have shown no benefit of immediate chemotherapy when compared with a watchful-waiting approach, so chemotherapy is typically deferred until disease progression. Rituximab (when used with the CHOP chemotherapy regimen) has become the standard of care for NHL, so looking at it’s activity in another lymphoma subset makes sense.
What I love about this compound:
Anything that significantly delays disease progression without the side effects of chemotherapy would be a welcome addition to treatment options in FL.
8. Concomitant VEGF and MEK inhibition
There are a couple of novel approaches looking at new combinations at the ASH meeting. Thoughtful research studies can often inform us about a potential new approach that might be worthwhile considering in the clinic. One such example I came across was dual VEGF and MEK inhibition in pediatric 11q23 AML. In AML, it has been found that simultaneous activation of these pathways results in a poor prognosis, so this would be a logical therapeutic combination to consider in appropriate children. Chromosomal translocations involving the Mixed Lineage Leukemia (MLL) gene at locus 11q23 are also associated with a poor outcome. These translocations represent approx. 15-20% of pediatric AML.
What I love about this concept:
As a result of the preclinical research, future studies looking at a VEGF-MEK combination are now being planned in pediatric AML and will be worth watching out for.
9. Panobinostat and everolimus (Novartis)
Believe it or not, I was actually trying very hard to avoid selecting another Novartis drug or combination, but they have a very broad portfolio in oncology and lots of interesting early data coming out. The reasoning behind this combination is that mTOR and deacetylase (DAC) inhibitors have demonstrated single agent activity in patients with relapsed and refractory lymphoma. Synergy between DAC inhibitors and mTOR inhibitors has also been observed in lymphoma cell lines in vitro. This is a phase I dose finding trial, so the results will be preliminary, but we should see whether the promise is possible from the early signals.
What I love about this concept:
HDAC and mTOR is a highly logical combination to explore in lymphomas based on the preclinical research to date.
10. TET2 mutations in myeloid malignancies
In case you’re thinking this might be a bit obscure, this presentation actually kicks off the Plenary session on Sunday and I have to say that it’s cool to see a Masters student present some really cool research.
“TET2 mutations are frequently found across broad spectrum of myeloid malignancies but how these mutations contribute to diseases is still unknown.”
I’m not going to spoil the presentation, but what I suspect they may have is a new therapeutic target in myeloid malignancies based on a mutation that occurs through epigenetic changes.
To check out some other top lists, take a look at Dr Anas Younes Facebook page, where he has posted his top 10 lymphoma clinical abstracts. I haven’t seen any other 10 ten abstracts for ASH yet, so we may well be the first two to stick our necks over the parapet 🙂
Disclosures:
– I own no stock in any of these companies (perhaps I should!)
– I’m a former employee of Novartis who worked on imatinib and my company has done consulting work for them.
I’m currently wading through the ASH abstracts on leukemia, lymphomas and myeloma and probably won’t have time to put out a substantial post today. The meeting is only two weeks away, how time flies!
You can search and check out this year’s abstracts and schedule online here.
This year, I’m actually doing ASH in Orlando and then the San Antonio Breast Cancer Meeting back to back, what was I thinking? The good news is that the annual Hot Topics and pipeline posts for both events will appear here on the blog soon.
If there are any ASH abstracts on targeted therapies that you would particularly like discussed in a future post, please feel free to add your suggestions/requests in the comments below.
This is my second to last report on the interesting new data coming out from the American Society of Hematology (ASH) meeting in New Orleans, LA earlier this month. They've taken a little long than I expected to get through due to our current workload and client reports, so sincere apologies for the backlog.
The final update will be a comprehensive one on chronic myeloid leukemia (CML), but today I wanted to focus on myelodysplastic syndromes or MDS for short. Let's start with a basic question: what are they?
According to the NCI:
"The myelodysplastic syndromes (MDS) are a group of disorders characterized by one or more peripheral blood cytopenias secondary to bone marrow dysfunction. MDS are diagnosed in slightly more than 10,000 people in the United States yearly for an annual age-adjusted incidence of 3.4/100,000 people."
MDS can arise naturally or as a result of chemotherapy given to treat acute myeloid leukemia (AML). Unfortunately, secondary MDS has a much poorer prognosis than de novo.
lenalidomide for patients with deletions of chromosome 5q31.
A few years ago I remember sitting in a packed plenary session and getting goosebumps hearing about the lenalidomide data in patients with 5q31 deletions, or maybe it was the freezing hangar where the presentations were being held, but the science behind the concept was fascinating.
The question is, what was hot this year at ASH in MDS? Here's a roundup of some of the interesting data I thought was interesting and relevant to this disease:
Bortezomib (Velcade): This study suggested that Millennium's drug, currently approved for the treatment of myeloma and mantle cell lymphoma, may be effective in MDS. The study included 10 MDS patients with a median age of 64 years. Bortezomib was given at a dose of 1.3 mg/m² on days 1, 4, 8 and 11 every 28 days for a maximum of eight cycles. 6 patients completed all eight cycles. Of the 6 evaluable patients, 3 patients (50%) achieved a minor red blood cell response, and three patients (50%) achieved stable disease. 7 out of 10 patients survived to the median follow-up of 24 months.
Four patients experienced severe neutropenia (low white blood cell count), and six patients experienced severe thrombocytopenia (low platelet count). 7 patients experienced other non-blood cell-related side effects including diarrhea, fever, skin rash, and pneumonia.
It was concluded that single agent bortezomib has some initial efficacy in achieving hematological improvement in MDS patients but a larger sample of MDS patients is needed to confirm these results.
Lenalidomide(Revlimid): Some German researchers looked at gene expression profiles to try and predict responses to therapy in MDS. They found that single sample prediction could discriminate 3 out of 8 patients as possible responders to lenalidomide, but this was not correlated with the clinical course of those patients while on treatment with the drug. In addition, it appeared that none of the MDS-patients receiving lenalidomide showed significant clinical response as defined by reduction of transfusion requirement by 50% or transfusion independence. The researchers concluded that prediction of response to treatment with lenalidomide in patients with Non-Del 5q myelodysplastic syndrome by gene expression profiling remains difficult.
A phase III trial looked at the optimal dosing for lenalidomide in 205 patients wo were randomised to receive either 5mg or 10mg of lenalidomide versus placebo. Previous phase II trials have shown that lenalidomide resulted in transfusion-dependence (RBC-TI) in 67% of patients and complete cytogenetic response (CyR) in 45% of patients with RBC transfusion-dependent low or intermediate risk MDS with del5q.
The researchers concluded that both doses of lenalidomide were generally well tolerated and achieved significant transfusion dependence and CyR. Lenalidomide 10 mg was associated with better RBC-TI and CyR than 5 mg, while maintaining a comparable safety profile. The data supported the use of 10 mg as a starting dose, with dose reductions or discontinuations, if needed.
Arsenic trioxide (Trisenox): A phase II study investigated the combination of ATO and ascorbic acid is tolerable. The drug was administrated intravenously over 1 hour at the loading dose of 0.30mg/kg/day for 5 consecutive days, followed by 0.25mg/kg/day twice weekly for 15 weeks. Ascorbic acid 1000mg was given by IV within 30 minutes after each arsenic trioxide infusion.
44 patients were enrolled in the study and 10 obtained a response (23%), including 1 complete remission. In 8 out of 10 responders, the response was evident within the first 8 weeks of treatment. 52% patients discontinued treatment because of various factors including disease progression (11%), severe adverse events (32%), drug unrelated adverse events (5%) and withdrawal of consent (5%). Severe neutropenia and thrombocytopenia were observed respectively in 45% and 23% patients.
Overall, the researchers concluded that the combination of ATO and ascorbic acid was tolerable and active in about 25% of MDS patients. The addition of ascorbic acid to ATO does not increase neither the toxicity nor the response rate to ATO. The tolerability of this regimen is reduced in elderly and high risk patients.
Vorinostat (Zolinza): Merck's HDAC was initially approved for CTCL, a rare form of NHL, but we have seen little dramatic data from other clinical trials since. There is, however, significant logic in testing epigenetic therapy in MDS.
This phase I study looked at the combination of vorinostat with decitabine in the treatment of newly diagnosed AML or MDS using 6 different dosing schedules including concurrent and sequential therapy. 72 patients were entered into the study with a median age of 68 years and 58% were male. To date, 69 patients have discontinued. Of the 70 patients evaluable for safety, 69 experienced AEs, the majority of which were relatively mild ie grade 1/2 in severity and included nausea, diarrhea, fatigue, constipation, and vomiting. In MDS patients receiving concurrent therapy, complete remission (CR) was achieved in 2 out of 5 patients, stable disease (SD) in 1 patient, partial remission (PR) in 1 patient, and hematologic improvement in 1 patient; all 6 of the patients who received sequential treatment experienced SD.
Overall, although preliminary, the data is promising and indicates that the combination of vorinostat and decitabine, either concurrently or sequentially, is possible without significant toxicity.
In all, while MDS is a particular difficult to treat disease, the initial results suggest that further investigation of drugs such as bortezomib, lenalidomide, arsenic trioxide and vorinostat is warranted and if further studies show more durable and repeatable responses, we may potentially see some new treatment options for MDS in the near future.
It was interesting to see exhibitors at the recent American Society of Hematology meeting place conspicuous signs in booths that had a café, alerting health care professionals that they should not ask for a free cup of coffee, tea or water if their licensing State, Government or Institution prohibited them from doing so.
Massachusetts and Vermont are two states that have recently banned health care professionals with prescribing authority from accepting anything of value directly from a pharmaceutical or medical device manufacturer including food & drink where the gift is linked to promotional activities. Other states such as New Jersey may soon follow suit.
Manufacturers are businesses with products to promote. They try and attract health care professionals to stop by their exhibits by offering information, and in some cases comfortable seating or refreshments such as biscotti or small ice cream. Nobody raises any questions about the subsidy to the meeting costs that exhibitors effectively provide, yet the offer of a coffee, tea or water at a booth that a doctor, nurse or physician’s assistant voluntarily chooses to visit is now regarded as a “gift” that several states have banned.
To me, the pendulum has swung too far in the regulation of pharmaceutical promotional activity if people really think a health care professional is induced to prescribe based on a free coffee at a conference exhibit booth. It is rather insulting if regulators think a doctor can be so easily bought.
If fewer health care professionals visit the booths due to lack of chotckhes or refreshments, the day may well soon come when exhibitors begin downsizing their booths and paying less for the privilege. The end result in the long run may well be higher registration fees for all, including physicians.
Perhaps there should be a minimum value of “gift” that is regarded as ‘de minimis’ and exempt from oppressive regulation. Long live free coffee at conference exhibit booths!
At the American Society of Clinical Oncology (ASCO) meeting earlier this year, we learned that rituximab added to standard fludarabine plus cyclophosphamide improved overall survival in patients with chronic lymphocytic leukemia (CLL), even in elderly patients of 70 years old.
Six months later, one of the highlights of the American Society of Hematology
(ASH) meeting held in a rather cold, wet and windy New Orleans, was updated data presented by
the same German CLL Study Group (GCLLSG) confirming the combination of
fludarabine, cyclophosphamide and rituximab (FCR) as the current front-line
standard of care in chronic lymphocytic leukemia (CLL).
Michael Hallek of the University of Cologne reviewed updated results from the GCLLSG CLL8 study, in which FCR was compared against the combination of fludarabine and cyclophosphamide (FC). At ASH in 2008, data was presented showing FCR to be superior to FC in terms of response rate and progression free survival (PFS). This year at ASH, Hallek presented updated data showing that patients in the FCR study arm still had a statistically significant higher overall survival (OS) compared to those receiving FC.
The published abstract shows the OS rate at 37.7 mo was 84.1% in the FCR arm versus 79.0 % in the FC arm (p=0.01). At the conference, Hallek presented data showing an 87.2% OS in the FCR arm versus 82.5% in the FC arm (P=0.012) at three years for those who achieve a complete response. There is a clear survival benefit from treatment with FCR as compared to FC, particularly in those patients who have Binet A or B stage disease.
The data for this combination suggested that it appears to be safe and effective. Response rates for BR were similar to those obtained with FCR. However, there were significantly less neutropenias with BR than would be expected with FCR. This has led the GCLLSG to initiate a protocol (CLL10) comparing FCR against BR in front-line CLL. The results from this study will show whether the new standard of care in front-line CLL should become bendamustine in combination with rituximab in the future.
In the poster sessions, a number of interesting ones jumped out at me that may be worth looking at in the clinic for the future.
Lenalidomide (Revlimid) has shown early promise in CLL in the CLL5 AGMT study. This was a phase I/II study that looked at combining fludarabine with rituximab with escalating doses of lenalidomide. Although only a small number of evaluable patients (n=6) were available, all 6 patients responded and 3 achieved a complete response. 40% of the patients were dose limited due to skin and vascular toxicities so the protocol was amended to include thrombo-prophylaxis and delayed start of prophylaxis against pneumocystis. It is too early to tell whether this regimen will reach the prime time but the risk-benefit trade-off may turn out to an issue.
An interesting compound that I have been following for a little while is Trubion's TRU-016, which is a small modular immunopharmaceutical protein (SMIP) being tested in relapsed and rferactory CLL. It targetes CD37, expressed predominantly on B-cells. In a phase I study, interim results were presented from CLL patients (n=33), demonstrating a manageable safety profile despite grade 3/4 myelosuppression. The DLT and MTD had not yet been reached. Reductions in peripheral lymphocytosis were observed, together with some objective responses in the higher dose cohorts. hopefully, further data will be available on this novel agent at ASCO in the summer.
Overall, with new monoclonal antibodies in development and the recent approval of ofatumumuab in refractory CLL, it is likely there will be interesting new data and further changes to the standard of care over the next two or three years. Biomarkers are also slowly emerging in CLL research, and while it is early days yet, it is good to see some attention finally being given some importance in this disease both from a predictive and a prognostic standpoint.
We can expect some compelling new data in the treatment of CLL, hopefully by ASCO in June 2010.
Acute myeloid leukemia (AML) is a truly nasty disease and one I hope never to have the misfortune to be diagnosed with.
Last month, at the Chemotherapy Foundation in New York, Dr Norman Wolmark gave an entertaining lecture on what he called the "Decade of Discontent" in colorectal cancer, a bleak period where no new therapies or stunning ideas emerged and the researchers bogged themselves in answering minutiae rather than focusing on the bigger picture.
He could well have been describing AML.
Why?
Take a look at this slide that was shown at the AML Super Friday educational symposium (the reference is from Dohner et al., (2009), published in Blood and how complex the disease has become with a myriad of phenotypes being described:
But this approach begs a most important question:
Which of these mutations or phenotypes are actually relevant and what is driving the cancer's survival and ability to outwit treatment?
No one really knows and thus it illustrates the frustration inherent in making a nasty disease ever more complex. Just because a mutation exists or a pathway is overexpressed does not mean that it is critical to the survival of the leukemia cells! Sometimes the mutations occur as artifacts, a function of a generally increasing leukemic burden over time as the disease gets more established.
Undoubtedly, the 14% of AML patients who have no additional mutation beyond the t(9,11) translocation that defines the disease, probably do best and at least attain a complete response (CR). The issue of how to keep them there, thus preventing relapse from occurring is an entirely different matter. We need more smart young researchers like Dr Gail Roboz in New York who asked the Chemotherapy Foundation audience what can be done to keep more AML patients in remission?
In ALL, which is more common in children than adults, there are well accepted maintenance therapy strategies for maintaining remission. In AML, post transplant or chemotherapy, there are none. Why it is not clear, but certainly something that can be easily tested with the plethora of targeted agents we have available on the market or in the clinic.
At the American Society of Hematology meeting in New Orleans this week, we attended a number of education and oral sessions discussing AML and read many posters on the topic too. What was startling was how little real progress has been made over the last five years… there were numerous versions of induction and conditioning regimens associated with stem cell transplantation, a general agreement that using the current targeted agents in late stage relapsed or refractory disease is doomed to failure because the leukemic burden is too high…
Dr Wolmark's 'decade of discontent' comment rang loudly in my ears while walking around a huge cold hangar on Monday reading poster after poster with little positive news to inspire or encourage. Skipping to the CML, CLL or NHL poster sections brought cheer and hope by comparison.
Part of the problem with AML is that many of the patients are diagnosed in the elderly, thereby limiting options either because the regimens are highly toxic and less well tolerated, transplant is not an option (survival decreases in the over 55 yo) or they have co-morbidities and multiple mutations, reducing the effectiveness of therapy.
There is, therefore, a clear need for alternative approaches in this population as well as better therapies for the very young who at least have a chance of cure by preventing relapse.
At ASH, some abstracts did catch my eye. Genzyme's clofarabine (Clolar) is one such interesting drug, currently approved for acute lymphocytic leukemia (ALL) and being tested in elderly AML patients. FDA's ODAC recently declined to approve clofarabine in elderly AML patients in the relapsed/refractory setting because the trial was compared to placebo. The same thing happened with Vion's laromustine (Onrigin) in the elderly AML setting. We will probably have to wait until the comparative trial data is available for clofarabine in 2010 before any major decision can be made as to the drug's safety and efficacy in the elderly population. There were no new abstracts on laromustine at this ASH meeting.
Meanwhile, some other interesting companies with early phase I/II data in AML included Sunesis and Cyclacel, both of which have seen their stock price rise since ASH on publication of the data.
Sunesis are developing voreloxin, a chemotherapy given as an infusion and used either alone or in conbination with cytarabine (araC) in heavily pre-treated AML. In the combination study (#645), the researchers found that:
"Among evaluable first relapse (n=36) and primary refractory patients (n=28), preliminary median overall survival is 7.8 months and the remission rate is 31% (complete remission [CR] 27%, complete remission without full platelet recovery [CRp] 2% and complete remission with incomplete recovery [CRi] 2%).
Historical median overall survival data in primary refractory and first relapse patients on currently available chemotherapies range from Voreloxin in combination with either bolus or continuous infusion cytarabine was generally well-tolerated. Infection-related toxicities were the most common Grade 3 or higher non-hematologic adverse events. In addition, Grade 3 or higher oral mucositis was observed."
A poster (#1037) was also presented on voreloxin in elderly AML, and while the data looks interesting initially, I would have major concerns about the registerability of the data given that it is a single arm study of the sort that the FDA and ODAC has repeatedly baulked at:
"Median survival was 8.7 months in Schedule A; 5.8 months in Schedule B; and 7.3 months (preliminary) in Schedule C (72 mg/m2 on days one and four).
Median duration of remission was 10.7 months and one year survival was 38% for Schedule A. For the other schedules, median duration of remission has not been reached and one year survival is too early to evaluate.
Patients age 75 or older (N=49) with at least 1 additional risk factor at diagnosis, a population identified by the National Comprehensive Cancer Network (2010) AML Guidelines as having poor outcome to standard treatment,experienced a CR rate of 30% and a 30-day all-cause mortality of 5%.
Survival in these patients was too early to evaluate.
Based on trial results, Schedule C has been determined to be the recommended pivotal dose regimen. For Schedule C, response rates (CR and CRp) are 38%; 30- and 60-day all-cause mortality are 7% and 17% with improved tolerability over Schedule A."
Cyclacel is a NJ biotech developing an oral prodrug for AML, MDS and CTCL called sapacitabine, a nucleoside agent that targets DNA synthesis and cell cycle arrest. Several phase II studies were presented at ASH, including interesting data on long term follow up in elderly AML patients from an MD Anderson study (#1061) and another in MDS (#1758).
It should be noted that while the one-year follow up data looks promising in AML, the study design suffers from the same issue as tipifarnib, clofarabine, laromustine, and voreloxin in that there is no comparator arm from which to compare and determine if the investigational agent is actually significantly prolonging life in AML.
Overall, it was a disappointing meeting in AML and I sincerely hope that some mre enlightening data emerges in 2010 rather than face the dreaded precipice that Wolmark so pithily described.
In the past, single agent and double agent regimens have been a mainstay in the treatment of multiple myeloma, yet the five year survival rate has remained steadfastly low around 3-4 years, on average. Typically, younger and fitter patients do better than elderly patients with a poorer performance status, yet the majority of new diagnoses are found in the elderly. Finding new treatment approaches is therefore a key imperative.
2009 has seen the advent of new triple, and even quadruple, combinations in an effort to improve efficacy and survival, hopefully not at the expense of increased side effects. Two of the most commonly used drugs, bortezomib and lenalidomide, for example, differ in their side effect profile with an increased
tendency to peripheral neuropathy and deep venous thrombosis,
respectively. New dosing regimens have begun to look at new strategies in the form of modified dosing regimens, which are potentially more patient friendly, without compromising efficacy.
Important trial results from two European groups at this American Society of Hematology (ASH) meeting, for example, demonstrated that a four
drug combination improved durable responses and progression-free survival in
elderly patients. Both studies showed that a
weekly schedule of bortezomib (Velcade) maintained efficacy with fewer toxic side effects (i.e. significantly decreased the incidence of grade 3-4 peripheral neuropathy) compared to the standard
twice weekly schedule.
In
newly diagnosed myeloma patients the combination of bortezomib with
melphalan-prednisone (VMP) has been previously shown to be superior to MP, while in relapsed-refractory patients the four drug combination bortezomib-melphalan-prednisone-thalidomide (VMPT) induced a high
proportion of complete responses (CR).
An Italian phase III study therefore looked at the four drug combination in the upfront setting and showed that induction therapy with a four drug combination of bortezomib,
melphalan, prednisone, and thalidomide (VMPT) followed by maintenance
therapy with bortezomib and thalidomide (VT) achieved superior response rates and PFS compared to VMP.
A Spanish study noted that previously in elderly patients with newly diagnosed myeloma, the VISTA
trial demonstrated that the combination of bortezomib plus
melphalan – prednisone (VMP) is significantly superior to MP alone.
However, it is unclear which agent is the optimal partner
for bortezomib: an alkylating agent or an immunomodulatory drug, so they set out to answer this critical question by comparing VMP to VTP, where T is thalidomide.
The results indicated that:
"1. Both modified induction schedules (VMP and VTP) are highly effective with similar ORR and CR rates, but a
clear different toxicity profile (more neutropenia, but less cardiac
toxicity and peripheral neuropathy with VMP)
2. Maintenance therapy with either VT and
VP markedly improve the quality of responses with a good safety
profile
3. The combination of these induction and
maintenance schedules seems to overcome the poor prognosis of high-risk cytogenetic abnormalities in elderly MM patients"
It should be noted that while melphalan causes more neutropenia, the cardiac toxicity seen with thalidomide is more difficult to manage, so the VMP combination is likely to be more suitable going forward in newly diagnosed elderly patients with myeloma.
One triple combination that garnered a lot of interest earlier this year at ASCO, was a trial looking at combining lenalidomide (Revlimid), bortezomib (Velcade) and dexamethasone (RVD) in relapsed or refractory myeloma patients, with overall response rates (ORR) of 69%, including 26% complete/near complete responses (CR/nCR) and manageable toxicities Anderson et al. ASCO 2009). The phase I portion of the study (Richardson et al. IMW 2009) found the maximum tolerated dose (MTD) of this combination in newly diagnosed myeloma patients to be lenalidomide (25 mg/day), bortezomib (1.3 mg/m2), and dexamethasone (20 mg). In all phase I patients, the ORR was 100%, including 31% CR, 9% nCR, and 75% very good PR (VGPR).
At this ASH meeting, we heard results reported for patients treated in the phase II portion of the study as conditioning prior to autologous stem cell transplantation (ASCT) by Dr Richardson, who concluded that:
"These phase II results suggest that RVD is a highly
effective combination, with a pre-ASCT ORR of 100% and high rates of CR/nCR, and encouraging time-to-event analyses to date. RVD
was well tolerated, with limited rates of grade 3 peripheral neuropathy and DVT/PE despite
prolonged use of bortezomib and lenalidomide."
The data are summarised in the table below, based on all patients (n=35):
Patients
ORR, %
CR/nCR, %
≥VGPR, %
Response at cycle 4 (n=31)
78
12
12
Response at cycle 8(n=24)
100
33
67
Best response
100
54
69
Some of the most exciting new developments in myeloma could be found in both the oral and poster sessions.
A new generation proteasome inhibitor, carfilzomib (PX-171), has been generating consistent results in the bortezomib refractory setting. An ongoing phase II study presented at ASH looked at carfilzomib monotherapy in myeloma patients with relapsed or refractory disease following 1–3 prior therapies, ie a heavily pre-treated population. Updated data for the bortezomib-treated cohort were reported at ASH and the authors concluded that:
"18% ORR (CBR 30%) is notable for this steroid- and
anthracycline-sparing regimen. Single-agent carfilzomib is well tolerated, even
in patients with renal insufficiency, and both myelosuppression and peripheral neuropathy
are uncommon."
Carfilzomib was originally developed by Proteolix, who have just been acquired by Onyx. This should ensure more solid funding for the development of the phase III program, which looks promising in the relapsed, refractory setting.
Perifosine (Keryx) modulates Akt, and a number of other signal transduction pathways,
including the JNK and MAPK, all of which are associated with programmed cell death, cell growth, cell
differentiation and cell survival. Updated data from a phase I/II study in 84 patients who were heavily pre-treated with a median of 5 prior lines of therapy (range 1-13), showed that the overall response rate (ORR) was 41%, for the bortezomib relapsed group, 65%, and for the bortezomib refractory group, 43%.
Approximately 60% of patients
demonstrated progression (or stable disease (SD) for 4 cycles) at some point in their
treatment and received 20 mg dexamethasone, four times per week, in
addition to perifosine plus bortezomib. Responses occurred both with
patients taking perifosine in combination with bortezomib and with
patients receiving the combination plus dexamethasone. The ORR for the perifosine plus bortezomib arm was 25%, with an increase to 38% when dexamethasone was added. Survival data in the 73 evaluable patients was 6.4 months for PFS and 25 moths for overall survival (OS).
Another exciting new compound in development is MLN4924 from Millennium, the novel mechanism of which was recently described in detail (see article below) and was the also subject of a Nature article. The compound works very differently from proteasome inhibitors, which target the proteasome substrate. MLN4924 is involved with neddylation rather than direct ubiquination.
Neddylation activating enzyme (NAE) is the E1-activating enzyme for the ubiquitin-like protein Nedd8.
NAE catalyzes the first step in the neddylation cascade leading to
modification of cullin-based ubiquitin ligase activity. This results in
specific protein substrates, with important roles in cancer cell
survival, being targeted for degradation as shown the diagram below:
Source: Soucy et al., 2009
The end result is that MLN4924 inhibits neddylation by disrupting the cullin-RING ligase-mediated protein turnover, leading
to apoptotic death in human tumour cells by a new mechanism of action,
the deregulation of S-phase DNA synthesis.
A phase I dose escalation study in myeloma and NHL patients with MLN4924 was reported at ASH. The primary objectives were to determine the maximum
tolerated dose (MTD) and safety profile of MLN4924, as well as describe the
pharmacokinetics (PK) and pharmacodynamics (PD) in blood. Among the 22 patients enrolled to date, the median age was 65 years, 14 had myeloma and 8 had NHL.
The results showed that NEDD8-Cullin levels in peripheral blood myeloma cells (PBMCs) were inhibited and Nrf-2 target gene
transcripts in whole blood were higher vs. baseline after MLN4924
administration, which is indicative of NAE inhibition. Cdt-1 and Nrf-2 levels in skin increased above baseline following the
second dose of MLN4924, which is indicative of NAE inhibition in peripheral
tissue. These results are promising and provide early proof of concept for the role of neddylation in myeloma.
Overall, this was a good meeting on the myeloma front with lots of promise for triple and quadruple combinations, as well as new agents being developed in both the newly diagnosed and refractory settings that augers well for the future, both in terms of improved survival and also more tolerable regimens.
Soucy, T., Smith, P., & Rolfe, M. (2009). Targeting NEDD8-Activated Cullin-RING Ligases for the Treatment of Cancer Clinical Cancer Research, 15 (12), 3912-3916 DOI: 10.1158/1078-0432.CCR-09-0343
Soucy, T., Smith, P., Milhollen, M., Berger, A., Gavin, J., Adhikari, S., Brownell, J., Burke, K., Cardin, D., Critchley, S., Cullis, C., Doucette, A., Garnsey, J., Gaulin, J., Gershman, R., Lublinsky, A., McDonald, A., Mizutani, H., Narayanan, U., Olhava, E., Peluso, S., Rezaei, M., Sintchak, M., Talreja, T., Thomas, M., Traore, T., Vyskocil, S., Weatherhead, G., Yu, J., Zhang, J., Dick, L., Claiborne, C., Rolfe, M., Bolen, J., & Langston, S. (2009). An inhibitor of NEDD8-activating enzyme as a new approach to treat cancer Nature, 458 (7239), 732-736 DOI: 10.1038/nature07884


![Reblog this post [with Zemanta]](http://img.zemanta.com/reblog_e.png?x-id=70ce2f9c-3c82-4c90-b7c6-846ef429870a)
![Reblog this post [with Zemanta]](http://img.zemanta.com/reblog_e.png?x-id=370caa1d-a6e6-43c9-8bf2-55b6785ccf29)

![Reblog this post [with Zemanta]](http://img.zemanta.com/reblog_e.png?x-id=a619c87d-96a3-4439-87ca-7e674892529d)
![Reblog this post [with Zemanta]](http://img.zemanta.com/reblog_e.png?x-id=6947f12b-c757-4c7c-bd66-32f2f07eb34f)