Developing a predictive biomarker for PARP inhibition
Today’s Science Friday post looks at the identification of a potential new biomarker and possible strategies for expanding use of PARP inhibitors in patients most likely to respond to them as a way to validate the the approach prospectively. This has important implications for future clinical trial designs with this class of drugs.

Photo Credit: Ben Sutherland via flickr
Regular readers will be very familiar at my rants against broad catch-all studies and phase III trials with targeted agents that do not have a biomarker or even a logical well defined subset of patients because it’s akin to blindfolding an archer, turning him around 360 degrees and then asking him to hit a bullseye 50 or 100 yards hence.
How can you hit a target you can’t see?
PARP inhibitors have had a bit of a chequered history after the initial excitement was later followed by a series of rather disappointing clinical trial results, which occurred for a multitude of reasons. Several of the approaches sadly fell into the category of ‘Five things not to do in R&D’ as delineated in my recent tongue-firmly-in-cheek post on the topic. I’ll leave interested and curious readers to ponder at length exactly which of the no-nos they managed to break!
That said, we do know a few things of relevance:
- PARP1/2 inhibitors have produced sustained anti-tumor responses in patients with germ-line BRCA gene mutations
- Biomarkers other than BRCA1 and BRCA2 are clearly needed to predict responses to PARP inhibitors
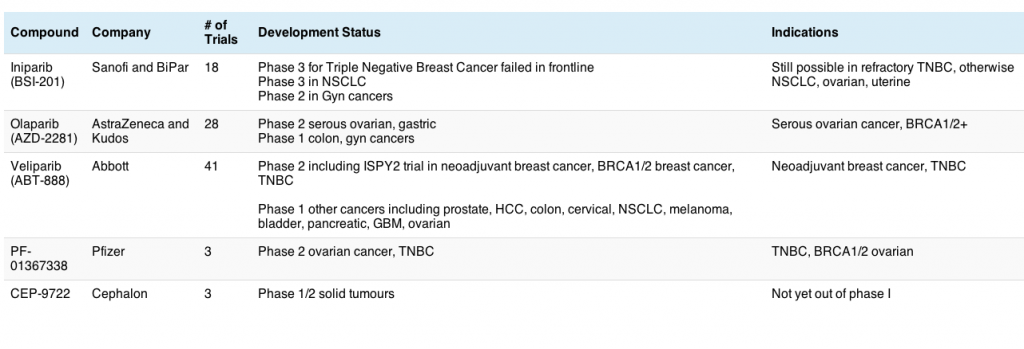
- Catch-all trials without segmenting for BRCA mutations and biomarkers are highly unlikely to be successful (recall the spectacular phase III failure in triple negative breast cancer with iniparib, for example)
- Next generation PARP inhibitors have focused on more clearly defined subset populations with greater success (and potency).
Chris Lord and Alan Ashworth’s lab have recently published some nice work (open access, see Refs below) that is worthy of discussion. Bajrami et al., (2013) decided to dive a little deeper and look at what genes and mutations might affect the responses to PARP inhibition:
“In hypothesizing that additional genetic determinants might direct use of these drugs, we conducted a genome-wide synthetic lethal screen for candidate olaparib sensitivity genes. In support of this hypothesis, the set of identified genes included known determinants of olaparib sensitivity, such as BRCA1, RAD51 and Fanconi’s anemia susceptibility genes.”
The main reason behind this approach quickly becomes apparent – there is a huge need for it:
“One of the major issues in the clinical development of PARP1/2 inhibitors is the identification of biomarkers other than BRCA1 and BRCA2 gene mutations that predict a favourable response to therapy.”
While patients with germline BRCA mutations have a greater tendency to respond, they don’t account for all the responses that have been seen in the clinic. What else is involved?
What did they find?
“Integration of the list of candidate sensitivity genes with data from tumor DNA sequencing studies identified CDK12 deficiency as a clinically relevant biomarker of PARP1/2 inhibitor sensitivity.”
In other words, when CDK12 was low, PARP sensitivity was high, making it a potential predictive biomarker for response to therapy with a PARP inhibitor.
What does this mean?
“The appearance of CDK12 in our olaparib sensitization gene list, alongside the CDK12 mutational data, suggested the possibility that loss of CDK12 function could sensitize tumor cells to PARP1/2 inhibitors and that loss of CDK12 function in HGSOVCa could be a predictive biomarker for response to this developmental class of agents.”
In other words, it would be useful to evaluate loss of CDK12 as a biomarker of response for PARP inhibitors in prospective clinical trials in breast and ovarian cancers, with and without germ-line BRCA mutations.
CDK12 is only one of nine genes known to be mutated in high grade serous ovarian cancer (HGS-OVCa), for example, so should patients be identified upfront who have loss of CDK12, then it may be enough to ensure response to a PARP inhibitor, irrespective of BRCA status. Clearly this work is still very early, but it creates a smart and well argued rationale that can be tested in clinical trials.
Should the approach be validated, then it could well expand the utility of PARP inhibitors in the clinic based on a predictive biomarker. I would be interested to see what happens not only with olaparib, but also the new generation of PARP inhibitors from Abbott (veliparib), Biomarin (BMN 673) and Clovis (rucaparib), to name a few who are conducting trials in breast or ovarian cancers.
If this works, it will be a thing of beauty.
References:
![]() Bajrami I, Frankum JR, Konde A, Miller RE, Rehman FL, Brough R, Campbell J, Sims D, Rafiq R, Hooper S, Chen L, Kozarewa I, Assiotis I, Fenwick K, Natrajan R, Lord CJ, & Ashworth A (2014). Genome-wide Profiling of Genetic Synthetic Lethality Identifies CDK12 as a Novel Determinant of PARP1/2 Inhibitor Sensitivity. Cancer research, 74 (1), 287–97 PMID: 24240700
Bajrami I, Frankum JR, Konde A, Miller RE, Rehman FL, Brough R, Campbell J, Sims D, Rafiq R, Hooper S, Chen L, Kozarewa I, Assiotis I, Fenwick K, Natrajan R, Lord CJ, & Ashworth A (2014). Genome-wide Profiling of Genetic Synthetic Lethality Identifies CDK12 as a Novel Determinant of PARP1/2 Inhibitor Sensitivity. Cancer research, 74 (1), 287–97 PMID: 24240700
Photo Credit: Ben Sutherland
 ASCO president, Dr George Sledge of Indiana, announced that the meeting theme for this year is “Patients, Pathways, Progress” to reflect the growing focus on molecular targets to identify and treat patients more effectively.
ASCO president, Dr George Sledge of Indiana, announced that the meeting theme for this year is “Patients, Pathways, Progress” to reflect the growing focus on molecular targets to identify and treat patients more effectively.